Biomedical Science and Research Journals | Treatment for Colorectal Cancer: Robot-assisted vs Laparoscopic Surgery
Treatment for Colorectal Cancer: Robot-assisted vs Laparoscopic Surgery
Abstract
Over the past few years, Robotic surgery has been an emerging field in colorectal surgery. Over years there has been continuous shift towards minimally invasive procedures with enormous potential advantages, but progress is impeded because of limited evidence, lack of technology and cost of expenditure. However, recent advances and feedback in robotic surgery and single-port incision in laparoscopic surgery are likely to improve surgical outcomes for treatment of colorectal cancer. Currently, laparoscopic surgery is preferred for colorectal cancer over open surgery and its usefulness is unquestionable. Laparoscopic surgery has become the standard of practice for various digestive tract surgeries. Although, robotassisted is gold standard for various other procedures, more research is needed to prove its safety and efficacy in the treatment of colorectal cancer. Robotic surgery may overcome limitations of laparoscopic surgery such as assistant dependent camera movements, retraction issues, lack of userfriendly environment and rigid instrumentation. Prolonged operative time, learning time, increased expenses and more trauma to the patient and family are major drawbacks of robotic surgery. In recent years robot-assisted laparoscopic surgery has been increasingly applied, again with lack of comparison and evidence over conventional laparoscopic surgery. The aim of this study is to compare robotic-assisted surgery and laparoscopicassisted surgery for the treatment of colorectal cancer (CRC).
Keywords: Colorectal cancer; Complication; Estimated blood loss; Length of hospital stay; Network meta-analysis; Operation time
Introduction
Colorectal malignant growth is a disease that begins in the colon or the rectum. These malignant growths can likewise be named colon disease or rectal malignant growth, contingent upon where they begin. Colon malignant growth and rectal disease are regularly gathered together collectively as they share same features. CRC is the third most generally analysed malignant growth in men and the second in women, with 1.8 million new cases and very nearly 861,000 deaths in 2018 as indicated by the World Health Organization. Throughout the decade, open medical procedure was considered the far reaching and objective standard for treatment and medical procedure of colorectal malignant growth. The point of careful treatment is tumour size, lymphatic waste, lymph node resection alongside clear careful edges. [1-6] In recent years there have been changes towards minimally invasive procedures and techniques, including the widespread adoption of laparoscopy techniques as an alternative to treat colorectal cancer instead of open surgery.
Kitano showed that contrasted and open medical procedure, laparoscopic medical procedure was a standard treatment for colon disease with shorter emergency clinic remains, quicker recuperation, improved rate of wound contamination, and diminished ago ny [1,3, 5,7-10]. Alongside advantages comes the downsides which incorporates inflexible instrumentation, absence of representation, poor withdrawal abilities alongside camera help and absence of innovation [2]. Robotic surgery was developed to overcome the technical difficulties of conventional laparoscopy. Robotic surgery has been advantageous because of its 3-dimensional operating field, surgeon operated camera field for better visualization. In addition to that there are studies about robotic systems especially the da Vinci Xi – a robot performing colorectal surgery has been found to be better performing and more efficient over the conventional laparoscopic surgery. Almost most of the controversy surrounding the use of robotic surgery remains around the fact that robotic surgery has high expenditure and longer operative hours leading to trauma to patient and families and tiring to the doctor as well. However, further advancement in this field has been limited by a plethora of challenges that must be addressed, including difficult implementation, and still somewhat limited technologies [10-12].
Although the limitations of laparoscopic surgery are met by robotic surgery, but the question arises whether these advantages are enough to offset the cost of robots. Furthermore, there has not been enough research performed over the blood loss, hospital stay, complications of the procedures and recurrence rate comparing both robotic surgery and laparoscopy surgery. The advancement in robotic surgery has leads to shorter learning curve and has been showed beneficial in various gynaecologic surgeries but its advantages in colorectal surgery are still been controversial [3,4,7,13-15]. Also, studies are very weak comparing both techniques and better clinical and surgical outcomes of the same. This investigation means to compare robotic assisted and laparoscopic ways to deal with colon and rectal methods to illustrate any distinctions in results.
Methods
Data collection and analysis
This study was a systematic review of publications in PubMed, Embase, Web of Science and Cochrane Library databases and the Cochrane Library comparing laparoscopic and robotic assisted colorectal surgery procedures. Databases were searched irrespective of dates under the Medical title “Robotic colorectal surgery” “Laparoscopic colorectal surgery” and “Robotic versus laparoscopic colorectal surgery”. This study was a meta-analysis of several eligible studies from public resources, thus informed consent and approval were not necessary.
Inclusion criteria
Publications were fused into the examination in case they met the going with criteria: relative examinations taking a gander at laparoscopic versus robotic colorectal frameworks, paying little regard to type (e.g, right hemicolectomy, low principal resection, sigmoid resection); randomized controlled primers, controlled clinical fundamentals, or observational examinations, if they were close in nature; and [7] studies were included but not limited to estimated operative time, amount of blood loss, postoperative outcomes, operative complications and conversions.
Exclusion criteria
Studies were excluded if the studies had incomplete data or if the study cannot be statically analysed. Studies were also excluded on the basis if they were letter and comments. Also, the literature which included the same population demographics were also excluded. Only the literature which had complete results and include various demographics of population were included.
Operative Techniques
Laparoscopic surgery
Patient was placed in lithotomy position and general anaesthesia was induced and both arms were adjusted alongside the body. Patient was tilted about 15 degrees opposite to the side of the tumour i.e. left colon cancer patient will be tilted towards right side. The inflation of abdomen with CO2 is achieved (pneumoperitoneum) through inserting needle in a 1mm port near umbilical area. The insufflator is set to 12-14 mmHg. A 12mm port is inserted 2cm below the umbilicus. Another 8mm port is inserted under direct vision in the upper quadrant which will be used as Arm 1. Other two 8mm ports are placed 4cm away from the symphysis pubis and 5 cm away from the xiphoid process serving as Arm 2 and 3 respectively. One 12-mm port is set under direct vision in the left-lower quadrant, to some degree below average contrasted with one side spin umbilical line (SUL) and insignificantly sidelong to the other side MCL. The use of inferior contrasted with preferable dissection over ligate and division the ileocolic vessels (supply course and vein), right colic vessels (conductor and vein), and right piece of the inside colic vessels (hallway and vein, as vital) [1,8, 9,11,12,16-18]. After satisfaction of get together of the ileum, cecum, rising colon, and proximal transverse colon. The precedent is isolated through this damage and is transacted. Simultaneously12`wz, hand-sewn from beginning to end anastomosis was performed extra-corporeally [7,8,19,20].
Robotic surgery
Patient was placed in lithotomy position after induction of general anaesthesia. The careful framework comprises of a control module with a top quality, three-dimensional (3D) camera where the specialist sits and controls effector mechanical arms in an “ace slave”. Every framework has an endoscope and three to four effector arms that join Endo Wrist gadgets, or tradable instruments that can be controlled with more prominent mobility than the human wrist. [6-8,15,21] While new frameworks are as of now being developed and will probably result in both monetary and innovation rivalry, the da Vinci remains the pioneer in mechanical careful innovation. Mechanical autonomy enables the specialist to see 3D pictures, acquire better points with the expanded degrees of opportunity given by the EndoWrist, and control three distinct instruments at the same time [10,22] Laparoscopic surgery is attainable and totally tantamount to open medical procedure, with points of interest in postoperative entanglements and emergency clinic remain.
Rectal laparoscopic resection is additionally plausible, and the investigations performed to date recommend that short and longhaul results are practically identical to open medical procedure. Regardless of the upsides of the laparoscopic approach for colorectal restorative system, this procedure has a couple of limitations, for instance, loss of the 3D vision, obstacles in the open-door degrees of the cautious instruments, the escalation of the physiological tremor and the “support” sway [20,22]. Although robotic surgery provides surgeons with various advantages which make complex laparoscopic procedures like identifying important neurovascular structures and intra-corporeal suturing in a deep and narrow pelvis easier. The absence of near investigations among robotic and laparoscopic approaches in regard to explicit results, joined with the expense of new innovation like the da Vinci robot (Intuitive Surgical), is a restrictive factor for across the board selection of the robot in numerous medical clinic focuses [3,7,8].
Statistical analysis
The meta-analysis of activity time assessed blood misfortune, length of clinic remains and complexity, mortality, anastomotic spillage, wound contamination, dying, and ileus. Socioeconomics and other applicable information were gathered, including study configuration, number of patients who experienced mechanical systems, number of patients who experienced laparoscopic methods, tolerant age, weight file, quantities of people, history of stomach medical procedure, and sign for medical procedure. All information was removed from the articles’ content, tables, and considers and entered along with an electronic spreadsheet for examination. For constant results, mean net contrasts (benchmark to-treatment change in treatment bunch mirrors change in charge gathering) were utilized as essential results. For clear cut results, chances proportions were utilized to analyse the treatment impact. To evaluate distribution inclination, channel plots were built for every result. No noteworthy distribution predisposition was identified for any investigation result utilizing either measurable strategy. Furthermore, affectability examinations were directed by barring each investigation thusly, to assess its relative impact on the pooled evaluation [3,6-8,11,15].
Results
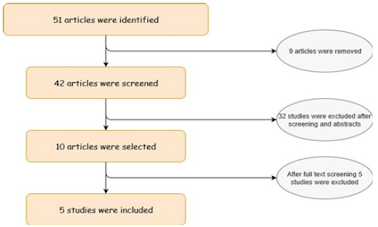
A total of 51 studies were identified and inclusion criteria was applied as illustrated in figure 1. After careful evaluation of titles, abstract, full text analysis and screening 5 studies were found to meet the inclusion criteria and were included for meta-analysis. A study which has a total of 1481 patients, out of which 807 patients underwent LACS and 674 underwent RACS. Another study was taken where 18 were right hemicolectomy, 1 sigmoidectomy, 3 abdominoperineal resection, 3 low anterior resection and 4 concomitant liver resections. Both the studies were used to compare Robotic and Laparoscopic methods of 2 different set of patients. [7,8, 23,24] Comparison of operating time, estimated blood loss, hospital stay, probability of complication, probability of anastomic leak and mortality for various patients is demonstrated in Figure 2. Calm measurement data and traits of the 2 clusters are seemed Table 1. There were no tremendous differences between the social events to the extent age, BMI, or history of stomach medicinal methodology.
The mean time of patients encountering laparoscopic restorative system versus mechanical therapeutic method was 61.1 ± 10.7 years versus 61.1 ± 8.5 years (P = .997), the mean BMI was 28.9 ± 6.3 versus 26.2 ± 4.2 (P = .158), and the rate with a past loaded up with stomach medicinal technique was 44.0% versus 26.7% (P = .273). There was a basic qualification to the extent sex, with more patients being male and encountering mechanized therapeutic method (86.7% versus 52.0%, P = .026). There was no significant qualification in cautious sign between the 2 social occasions (P = .303) [1,7,8,25,26]. Eighteen patients experienced right hemicolectomy, 1 encountered a sigmoidectomy, 3 experienced abdominoperineal resection (APR), and 3 experienced low front resection (LAR) performed laparoscopically.
Meta-Analysis
Estimated operative time
The value of operative time ranged between 1.00 to 1.01 good iterative effect and completely stable results. The result of meta- analysis presented in Figure 2(A) revealed that almost both laparoscopic and robotic surgery takes about the same amount of operative time with robotic taking a little more amount of time comparatively. [3,7,8,25,27] Although the relative difference between both is almost negligible.
Estimated blood loss
The analysis blood loss ranged from 1.00 to 1.01, proving nearly stable results as seen in Figure 2 (B). Result of meta-analysis reveals that comparative robotic surgery had more blood loss than laparoscopic surgery [1,7,8,27,28].
Estimated meta-analysis of length of hospital stay
The model of length of clinic stay had total assembly, great iterative impact, and stable outcomes. The consequences of the meta-examination uncovered that patients who experienced RACS had the briefest length of emergency clinic remain as illustrated in Figure 2 (C) [2,7,13-15].
Estimated rate of complications
The Figure 2 (D) suggests that the consequences of the meta-investigation uncovered that the inconvenience rate in patients who experienced RACS was the least, yet there was no huge contrast. [3,6,7,28].
Estimated analysis of mortality
The analysis of mortality went from 1.00 to 1.01, demonstrating total intermingling, great iterative impact, and stable consequences of the model as seen in Figure 2 (E). The outcomes demonstrated that the death rate in patients who experienced RACS was the least, yet there was no noteworthy distinction contrasted and those in patients who experienced LACS. [1,7,8,13,15].
Estimated analysis of anastomotic leak
The analysis of anastomotic spillage went from 1.00 to 1.01, showing total assembly, great iterative impact, and stable consequence of the model. Figure 2 (F) suggests these outcomes uncovered that the rate of anastomotic spillage in patients who experienced LACS was the least; however, there was no huge contrast contrasted and those in patients who experienced RACS [1,3,7,8].
Estimated analysis of wound infection and bleeding
The results revealed that the rate of wound infection in patients who underwent LACS was the least, but there was no significant difference compared with that in patients who underwent RACS. The result demonstrates that the rate of seeping in patients who experienced RACS was the least, yet there was no noteworthy contrast contrasted and those in patients who experienced LACS. The oncologic qualities of the colorectal undertakings performed for tumour resection were moreover noted (Figure 3). There was no tremendous difference in tumour sort out or histologic assessment between the 2 social occasions [1,7,8,22,23,26]. Furthermore, there were no basic differentiation in the amount of lymph centre points harvested between the laparoscopic gathering and the robotic surgery. No resections performed for damage yielded positive edges in either assembling.
Discussion
A network meta-analysis is performed comparing the curative effects of LACS and RACS in this study. Laparoscopic surgery has been widely accepted over open surgery for colorectal cancer. LACS has shown benefits and is also safer comparatively. For example, patients that have underwent laparoscopy surgery for colorectal cancer have demonstrated that it can yield a diminished length of hospital stay, oncologically sufficient resection, and no distinctions in postoperative stay [1,6,10,22,24]. In view of concentrates like these, laparoscopy is presently viewed as an adequate option in contrast to an open surgery in colorectal resection. However, conversion to open surgery still stays as a big pitfall for LACS. With the advent of new technology, RACS is now the growing field in medicine and is widely accepted for surgery in bariatric, urology, gynaecology and various other fields. [8,11,13,17,26]. The prevalence of RACS, one of the most recent advancements in laparoscopic medical procedure, has been expanding since it was first performed in cholecystectomy in 2001(Table 2).
The careful method is improved by the properties of the robot framework, for example, able to use both hands ability, 3-dimensional view, and tremor elimination. Similar to our examination, past investigations announced that RACS had the longest activity time [1,3,9,24,26]. However, it is important that the task time of RACS is negligible in progressively complex pelvic processes. However, the self-sufficiency of RACS is superior to that of LACS. A past report referenced that the expense of RACS was a lot higher than that of LACS. Also, it has been proposed that the length of medical procedure in the RACS was longer than that in the LACS gathering, while the quantity of lymph nodes collected, resection edge freedom, postoperative agony score, careful difficulties, and clinic stay were similar. The task times were accounted for to be altogether longer in patients treated with robots than that treated with lap aroscopy, though there were no contrasts between the 2 bunches as to entanglements and emergency clinic stay, which was like our outcomes. Two arrangement looking at RACS and LACS in right colectomy have shown that RACS has a more extended case time and higher all out medical clinic cost than LACS however comparative evaluated blood loss and length of emergency clinic stay.
It isn’t vital for RACS and LACS to change over to the open approach. Although there was no huge clinical preferred standpoint for RACS in assessed blood loss, length of emergency clinic remains, and confusion rate contrasted and LACS, the lymph nodes around primary veins could be cleaned effectively dependent on the steady camera stage [1,3-9,16,18,22] . In addition, RACS gave solace to the specialist by giving a superior usable act. Also, the conversion rate to open was very low in RCS compared to LACS, which proves as an added benefit. An exceptionally intriguing investigation from Kang et al, contrasted three gatherings of patients and mid and low rectal tumours treated with either open, laparoscopic or robotic methodology [14,21-23,27]. They saw that the robotic gathering had a quicker postoperative recuperation with a lower emergency clinic remain, less agony and better example quality. The sickness free survival rate was comparative in all gatherings three years after medical procedure [29]. A noteworthy debilitation for specialist’s keen on figuring out how to utilize a careful robot is the loss of touch vibe that is of huge significance in various methodology.
The activity of a specialist who can’t feel the distinctive tissues and strain turns out to be significantly increasingly troublesome, and the dangers of aperture and damage increment. Furthermore, while “hand-sewn” procedures are all the more promptly performed with apply autonomy over laparoscopy, the tissue pressure on the sutures should be accumulated from obvious signals. [7,8,13,28] These hindrances likewise exist in conventional laparoscopic methodologies and it is conceivable that new robotic innovation might almost certainly beat them. Despite the fact that this meta-analysis is extensive and the most present assessment of robotic and laparoscopic ways to deal with colon and rectal medical procedure to date, it ought to be deciphered with regards to some limitations [2-4,11]. This has various ramifications on the information, including consequences for the usable time and perioperative entanglements. Second, the scarcity of current randomized controlled preliminaries further constrains the consequences of meta-analysis. [3] Besides, not the majority of the investigations provided details regarding all results inspected inside this examination, prompting varieties in the included example sizes and factual power between results. Each investigation has its own inclinations and restrictions, with various incorporation and prohibition criteria, changing signs for medical procedure, and distinctive sorts of included colorectal strategies. [12,16,17,21].
Conclusion
Taking everything into account, the present system meta-analysis proposes that RACS may be a superior treatment for CRC. Robotic surgery would in general have longer operative time, less blood loss, and a lower rate of change to laparotomy compared to laparoscopic surgery. However, future examinations including forthcoming randomized controlled preliminaries and cost-adequacy is needed to decide if robotic surgery will have it say in colorectal techniques.
Acknowledgment
The author(s) declared that no grants were involved in supporting this work.
To view fulltext of article: https://biomedgrid.com/fulltext/volume4/treatment-for-colorectal-cancer-robot-assisted-vs-laparoscopic-surgery.000856.php


Comments
Post a Comment