Biomedical Science and Research Journals | Biomechanical Principles of Multipoint Suture Fixation for Abdominal Wall Reconstruction
Biomechanical Principles of Multipoint Suture Fixation for Abdominal Wall Reconstruction
Introduction
In the United States, approximately 400,000 ventral hernias are repaired every year with an estimated cost of about 3 billion dollars [1] . Ventral hernias are a relatively morbid condition given that an intact abdominal wall is necessary for dynamic activities such as rotation of the torso, respiration, defecation/urination, emesis, and childbirth.
The management of ventral hernias has evolved over the past several decades with advances in technology and knowledge. The first significant improvement was the use of prosthetic mesh reinforcement to simple suture repair alone [2] . As reported by Luijendijk, randomized controlled trials demonstrated a decrease in hernia recurrence rates from 43 percent to 24 percent [3, 4].
Another major advancement was the popularization of the component separation technique as escribed by Ramirez [5] . This technique was found to be particularly useful in the case of large hernias where primary closure of the hernia defect is not possible otherwise. In addition, it eliminates the need for prosthetic mesh and its associated risks, while providing comparable or superior reduction in hernia recurrence [6, 7, 8]. Perhaps more importantly, the component separation technique provides a dynamic abdominal wall reconstruction, using innervated muscle which is critical to reducing hernia recurrence. In addition, component separation procedures provide an anatomic alignment of the muscles, which enhances abdominal wall function.
The advent and implementation of biologic mesh or acellular dermal matrices (ADM) has offered an additional valuable tool in the reconstructive armamentarium for ventral hernias [9] . ADM is superior to prosthetic mesh in setting of contaminated and highrisk cases and is a valuable adjunct to the component separation technique [10, 11, 12]. Abdominal wall reconstruction with human acellular dermal matrices (HADM) has also been described [13] . However, since it has increase elasticity as compared to porcine or bovine ADMs, it can leave a significant bulge if used as an inter-positional bridge when myofascial continuity cannot be reestablished (Figure 1A) (Figure 1B)
Although component separation with biologic mesh reinforcement is effective, there is still not universal agreement as to the technique and location for mesh fixation [14].For standard mesh fixation, the retro-muscular or underlay placements are most commonly used and are associated with lower recurrence rates [15, 16]. There has been some difference in outcomes with different types of fixation for underlay indicating that the method of fixation is important [17] .Placement of sutures lateral to the junction of the linea alba and the anterior rectus sheath have been found to provide the greatest support and tolerance for tissue tension in studies on laparotomy closure [18] .
The multipoint suture fixation offers a technique that combines these advantages for the patient undergoing abdominal wall reconstruction for ventral wall hernia, including the largest and most complex hernias as well as those with infected mesh and soft tissue deficiencies. The multipoint suture fixation technique is a physiologic approach to hernia reconstruction. The technique utilizes wide exposure to avoid injury to the hernia sac or contents. In patients who have had a prior midline incision, that is used. However, in patients without incisions on the abdomen, an abdominoplasty type incision has been found to have a number of advantages [19] . Local anesthesia with epinephrine is injected along the planned incisions to minimize bleeding and facilitate the dissection. The hernia sac and defect are circumscribed, and dissection is continued cephalad to the xyphoid.
Component release incisions are made lateral to the lateral border of the rectus muscles to mobilize the rectus muscles to the midline. The location of the component release is determined by the width of the anterior rectus sheath. It is made at least 8 cms lateral to the midline inset of the rectus sheath. The fascia is released, and the external oblique muscle preserved. In patients in whom the loss of domain is greater, posterior release of the rectus sheath can be added as well. The two abdominal rectus muscles are brought together in the midline with several interrupted 0 Vicryl sutures to ensure alignment of the muscles. This is critical for two reasons, first as indicated previously, a lower recurrence rate is associated with patients in whom myofascial continuity is reestablished. Second, the proper alignment of is important for proper function of the muscles in the actions on the abdominal wall. Even a small deviation of the line of action can have a significant impact on the how effectively muscles function [20] . A looped 1 PDS is used as a continuous running horizontal mattress suture to imbricate the anterior fascia, which is the most effective suture technique [21] . This facilitates securing the anterior fascia just lateral to the junction of the linea alba and anterior rectus sheath where it is strongest [22] .
The intentional selection of HADM to reinforce the abdominal wall fascia offers several advantages. Fascia takes approximately two months to gain 40% of its original strength, but original strength is never regained [23] . The addition of HADM provides not only a temporary increase in tensile strength of the abdominal, but as it integrates, it reinforces the native abdominal wall structure.
As compared to non-crosslinked xenograft ADMs, HADM provide more rapid vascular ingrowth and integration and greater tensile strength of the musculo-fascial interface [24] . The HADM has greater elasticity than non-cross-linked xenograft ADMS or any of the crosslinked ADMs. While this elasticity is a disadvantage for standard inset or interposition graft placement, with the multipoint fixation it offers the advantage of increased abdominal wall compliance.
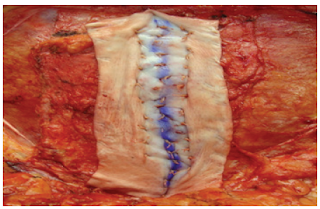
The wide exposure open approach facilitates careful placement of the HADM. It is secured along the midline imbrication to bolster the inset of the two rectus abdominus muscles. Additional sutures are then placed in an offset row pattern working from the midline out laterally in each direction. Progressive tension sutures have been well-described to fix soft tissue in abdominoplasties to decrease seroma formation [25] . With each row additional traction displaces the HADM laterally as compared to the underlying fascia. This helps fix the HADM to the fascia to decrease the risk of seroma formation between the HADM and the fascia. In addition, the number of sutures strands used for fixation had been demonstrated to have a critical effect on the strength of fixation [26] . Perhaps more importantly, each row progressively offloads the tension on the midline inset of the muscles.
This technique specifically addresses the underlying concept that recurrences most often occur at the mesh-fascia interface. The structural design provides maximum interface of the anterior rectus sheath and the HADM. The progressive tension sutures provide an increased number of fixation points and off-load the inset of the muscles. The clinical results of this technique show that a multipoint fixation suture technique for abdominal wall reconstruction with component separation and onlay biologic mesh is reproducible and effective with low recurrence rates.


Comments
Post a Comment