Biomedical Science and Research Journals | Sylvian Aqueductal Web/ Diaphragm-A Case Report and Short Review of Imaging Techniques
Sylvian Aqueductal Web/ Diaphragm-A Case Report and Short Review of Imaging Techniques
Abstract
Aqueductal Web/Diaphragm (AW/D) causing Aqueductal stenosis is a known but uncommon entity [1]. Appropriate diagnosis helps in prompt and adequate patient care. We present a case report of a 48 YOF who was evaluated for acute mental status changes with severe headaches. Regular CT images demonstrated obstructive hydrocephalus at the level of the Sylvian aqueduct. When an additional 10 minutes was spent on post processing using CT 3D Multiple Plane Reconstruction (MPR) function on a McKesson PACS radiology station, it showed an AW/D as the cause of obstructive hydrocephalus. As the patient was confused and couldn’t hold still, conventional MRI with 3D CISS sequince contained motion artifact, but still confirmed the finding.
Keywords: Aqueduct stenosis, Sylvian Aqueduct web, Sylvian Aqueduct diaphragm, Obstructive hydrocephalus, CISS-Constructive Interference in Steady State, CSF-Cisternography, McKesson PACS radiology station, Severe headaches, Neuroendoscopic aqueductoplasty, Visualizing cranial nerves
Abbreviations: AW/D: Aqueductal Web/ Diaphragm, YOF: Year-Old Female, CT: Computerized Tomography, MRI: Magnetic Resonance Imaging, CISS: Constructive Interference in Steady State, FIESTA: Fast Imaging Employing Steady State Acquisition, PACS: Picture Art-Chivying and Communication System
Case Report
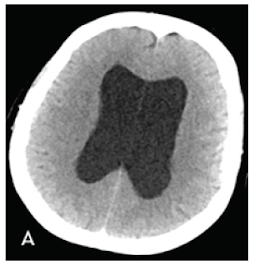
48 YOF came to the ER with acute mental status changes, severe headaches, nausea and vomiting. She had no significant past medical history. Regular CT images demon started obstructive hydrocephalus at the level of the Sylvian aqueduct. CT 3D sagittal reconstruction images demonstrated an AW/D. Extra Ventricular Drain (EVD) was placed in the ER and patient was admitted. MRI of the brain was performed with an additional CISS 3d sequence in a 3T Siemens Vireo magnet[2]. Sagittal and coronal reconstruction CISS images clearly demonstrated and confirmed the AW/D. EVD was Removed and endoscopic third ventriculostomy was performed with placement of a vein- triculoperitoneal shunt.
Imaging
CT Brain was performed using a 128 slice Siemens Somtam Definition Edge scanner. Axial images were obtained with 5mm and 1mm slice thickness. Using the 3D MPR function on McKesson Radiology PACS station, reconstructions were performed. The sagittal reconstruction images demonstrated obstructive hydrocephalus with AW/D (Figure 1B).
MRI brain was performed in a 3T Siemens Vireo magnet. The additional axial CISS 3D sequence was obtained with isotropic 0.6 x 0.6 x 0.6 voxels taking 7.18 minutes. Sagittal and Coronal reconstructions clearly demonstrated the AW/D Despite the Motion ArtiFact (Figure 2B) (Figure 2C).
Discussion
An AW/D is a congenital abnormality. The web is a translucent membrane composed of ependymal cells and fibrillary neuroglia [3] . In patients with prior subarachnoid hemorrhages, the linear structure could represent adhesions. Recognition of this entity facilitates surgical resection and cure instead of longterm shunting with associated complications. Neuroendoscopic aqueductoplasty [4] can be considered for restoring physiologic CSF circulation in carefully selected patients with Aqueductal stenosis [5, 6]. The 3D-CISS (Constructive Interference in Steady State) sequence on Siemens and FIESTA C (modified FIESTA Fast Imaging Employing Steady State Acquisition) sequence on GE are similar pulse sequences [7] . Because of its high spatial resolution, high signal to noise ratio and better differentiation between CSF and brain parenchyma it’s the current sequence of choice for CSFCisternography, visualizing cranial nerves, cavernous sinuses, small extra-axial lesions and ventricular system [8] .
Due to perfectly balanced gradients, it has inherent flow compensations. 3D-CISS sequence in our study took 7.18 minutes for acquisition. It has no adverse effects of radiation or an invasive procedure. CSF cine flow study is also used to show the degree of obstruction along the CSF pathway in conditions like Arnold Chiari malformation and Aqueductal stenosis. Time-resolved 2D phase contrast technique with velocity encoding, which depends on location specific sequential application of a pair of phase encoding pulses in opposite directions, is predominantly used to acquire CSF flow studies. However, it does not demonstrate anatomy of the obstructive lesions clearly. In our case report, the CT sagittal reconstruction images post processed on a McKesson PACS itself, demonstrated the lesion clearly. MRI study confirmed the finding.In patients with contra indications for MRI, CT 3D MPR is a good alternative.
Conclusion
It is known that 3D MPR CT images and 3D-CISS (Constructive Interference in Steady State) sequence, demonstrate aqueduct web/diaphragm in patients in a reliable and reproducible way. If the patient cannot hold still, a shorter sagittal thin section T2 slice sequence can be considered. However, in patients who have contraindications to MRI, adequately reconstructed sagittal images from 1mm CT axial images can also be used effectively to demonstrate the lesion.


Comments
Post a Comment