Biomedical Science and Research Journals | Fetal Cervical Teratomas: Etiology, diagnosis, and Treatment Options
Fetal Cervical Teratomas: Etiology, diagnosis, and Treatment Options
Introduction
Cervical teratomas are rare fetal tumors with a frequency of 1 in 20,000 to 1 in 40,000 live births, with a female-to-male ratio of 3:1 [1]. In a series of 1,253 teratomas of different types [2,3], only 6 (0.47%) were classified as epignathus [4]. Histologically, they are benign tumours formed by the three germ layers (ectoderm, mesoderm and endoderm). While the majority of fetal teratomas manifest themselves in the coccyx region, cervical teratomas represent only about 6% of congenital teratomas. Moreover, there are some cases in the literature where cervical teratomas showed a malignant tendency. Thus Thurkow et al. [6] reported an extremely rare case of malignant teratoma of the neck, with mature and immature metastatic lesions in the lungs, in an immature fetus [5]. Further, Bauman and Nerlich reported a metastazing cervical teratoma of the fetus [6]. Additionally, there is another report of six malignant teratomas in the literature so far [7].
Ultrasound diagnosis
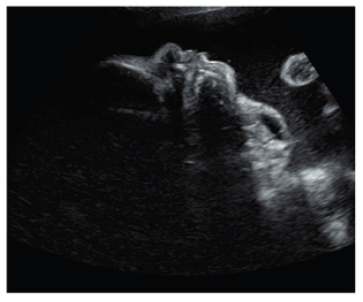
Ultrasound diagnosis has proved to be successful at very early stages of gestation. Thus between the 15-17 weeks an ultrasound detection can be achieved [8,9]. However, most of the lesions are seen in the late second and third trimesters, suggesting that the tumor can develop later in pregnancy [10]. The usonographic diagnostic clusters are based on the display of an anterior or bidirectional organoid facial mass that is partly solid and partly cystic (Figure 1). This mass protrudes (usually with no calcifications) from the fetal mouth and causes hyperextension of the head. Three-dimensional ultrasound can support the prenatal diagnosis [11]. Together with antenatal MRI, three-dimensional ultrasound may thus be of critical importance in identifying fetuses that require an ex utero intrapartum treatment (EXIT) procedure (Figure 1).
Prenatal treatment options
Cervical teratomas are rare congenital tumors with a poor prognosis and a nearly 100% mortality if not immediate managed and resected [12]. Teratoma occurring in the nasal cavity is a rare abnormality. When teratomas are found in the head or neck, high perinatal mortality occurs, mainly as the result of neonatal upper airway obstruction because the tumor impairs fetal swallowing and causes pharyngeal obstruction due to local mass effect. Thus, the main problems during pregnancy and the perinatal period are the increase in size, the resulting impairment of fetal swallowing with consecutive polyhydramnios and a significantly increased risk of preterm birth, and the difficulty of securing the airway postnatally [13,14].
For peripartal management, the decisive factor is whether there is compression of the upper airways. In these cases, delivery should be carried out by the so-called EXIT procedure (Ex Utero Intra Partum Treatment) in order to have sufficient time to secure the upper airways. This procedure, first described as a delivery method for fetuses with diaphragmatic hernia and iatrogenic tracheal occlusion [15], involves performing the dissection under general anaesthesia and high doses of inhalation anaesthetics for tocolysis. The edges of the uterotomy are secured with stacker systems to achieve the best possible hemostasis. After partial development of the fetus, the airways are secured at the placental perfusion. In collectives with fetal cervical teratomas, this part of the procedure takes 23 minutes [16,17] on average. The duration of placental support to the partially delivered fetus can even be as long as 60min [18]. A study reported the outcome of 23 EXIT procedures performed from 1996 to 2004 to deliver fetuses with giant masses in the neck. Three fetuses with giant cervical teratomas died of severe pulmonary hypoplasia. On postmortem, these patients presented severe airway distortion due to the mass. The carina was retracted superiorly to the first or second rib, resulting in compression of the lungs in the apices of the chest with pulmonary hypoplasia [19].
Disadvantages of the EXIT procedure are the risks of intubation anesthesia, increased maternal blood loss, and the increased risk of placental detachment, endometritis, and postpartum anemia [5]. A new alternative is fetoscopic endotracheal intubation (FETI) immediately prior to dissection, as described by Cruz Martinez et al [20]. This involves a fetoscopic endotracheal intubation (FETI) under local maternal anaesthesia. Using the Seldinger technique, an airlock is placed in the mouth of the fetus under ultrasound guidance and advanced through the fetoscope into the trachea. The free end of the endotracheal tube is placed in the amniotic cavity by slowly retracting the sheath and simultaneously advancing the sheath trocar under ultrasound control. Thus, the main disadvantages of the EXIT procedure can be eluded.
Conclusion
Cervical teratomas are rare, but usually benign congenital tumors with recognized multifactorial etiology. A prenatal ultrasound diagnosis can be made early in pregnancy (15-16 weeks) whereas 3D ultrasound and MRI may enhance the accuracy of the antenatal diagnosis and may aid in the selection of patients requiring treatment. The delivery of a fetus with a cervical teratoma should involve elective cesarean section with the EXIT or FETI procedure with a resection of the tumor mass afterwards.
For More information: https://biomedgrid.com/fulltext/volume9/fetal-cervical-teratomas-etiology-diagnosis-and-treatment-options.001422.php
Know More Information: Biomed Grid Please Click on : https://biomedgrid.com
For More information: Open Access Journals of Biomedical Science and Research: Journal of Biomedical Science
Know More Information: Biomed Grid Please Click on : https://biomedgrid.com


Comments
Post a Comment